Cannabinoid (CB) 2 receptor uptick likely occurs to protect cellular systems. CB2 receptors in the brain and gut adapt to specific cells following the loss of CB1 receptors. And a recent study assessed how cannabinoid two receptors treat spinal cord injury by recycling a critical inflammasome.
INFLAMMATORY INJURY AND ILLNESS
Earlier this year, Harvard Medical School released a pivotal study on Covid-19. The virus upticks an inflammasome, leading to a fiery cell death. I hypothesized an endocannabinoid deficiency, a major loss of 2-AG to be exact, as a crucial factor in the viral disease.
2-AG is a CB1 and CB2 receptor agonist. But cannabinoid two receptors are druggable targets that treat disease and injury caused by an inflammasome storm, including one induced by a spinal cord injury.
SPINAL CORD INJURY AND CANNABINOID RECEPTORS
According to a recent study, CB2 receptors help recycle the inflammatory protein known as NLRP3. The inflammasome remains inactive under homeostasis, a function of the endocannabinoid system. But if macrophage cells fail to clear toxins from the body, they warn the immune system, which releases NLRP3 proteins.
The process occurs in numerous diseases and leads to excessive cryopyrin. Proteins must degrade and properly recycle to avoid inflammation and pyroptosis, though. During spinal cord injury, CB2 receptor activation recycles inflammatory proteins via a unique enzymatic process — ubiquitination.
CB2 receptors, in part, boost a nutrient sensor axis (AMPK/ULK1) to recycle proteins. And NLPR3 inflammasome reduction, in turn, regulates neuron and epithelial cell polarity. CB2 receptor agonists can, therefore, regulate autophagy, prevent cell death, and attenuate neuroinflammation.
“NLRP3 inflammasome structure. The NLRP3 inflammasome is a complex consisting of NLRP3, ASC, and procaspase-1. NLRP3 consists of three regions: the pyrin domain (PYD) in the amino terminus, the NACHT domain, and the leucine-rich repeat domain (LRR) in the carboxy terminus.” — Seok et al. 2021.
A DRUG OR A TERPENE?
Beta-caryophyllene and delta-9 THC agonize CB2 receptors, but THC also targets the cannabinoid one receptor. Pharmaceutical companies failed to synthesize a selective CB2 agonist over the last decade.
The value of a functional and selective CB2 receptor agonist is in the billions, despite caryophyllene’s ubiquitous presence in our food supply. Drugs or terpenes that selectively target cannabinoid two receptors can treat various conditions, including Covid-19 and spinal cord injury, by recycling inflammatory proteins.
SOURCES EXPLAINING CANNABINOID RECEPTORS ROLE
Jiang F, Xia M, Zhang Y, et al. Cannabinoid receptor-2 attenuates neuroinflammation by promoting autophagy-mediated degradation of the NLRP3 inflammasome post spinal cord injury. Front Immunol. 2022;13:993168. Published 2022 Sep 26. doi:10.3389/fimmu.2022.993168
Sefik E, Qu R, Junqueira C, et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature. 2022;606(7914):585-593. doi:10.1038/s41586-022-04802-1
Seok, Jin & Kang, Han Chang & Cho, Yong-Yeon & Lee, Hye & Lee, Joo. (2021). Therapeutic regulation of the NLRP3 inflammasome in chronic inflammatory diseases. Archives of Pharmacal Research. 44. 10.1007/s12272-021-01307-9.
Cannabinol or (CBN) as it is called, is one of the most exciting minor cannabinoids in the cannabis plant. Much of the industry is focused on THC and CBD-based products, but research is slowly uncovering the significant therapeutic potential of minor cannabinoids like CBN on the human body.
How can CBN help medical patients? Does CBN get you high? What are the effects?CBN has many potential health benefits that can aid with everything, from insomnia to seizures and so much more. Here is what you need to know about this up-and-coming cannabinoid.
What Is this Cannabinol (CBN)?
Well CBN is a THC metabolite, for whatever that means. So in aged cannabis plants, tetrahydrocannabinol acid (THCA) degrades to cannabinolic acid (CBNA) when exposed to light and heat. Generally, cannabis plants contain trace amounts of CBN (under 1%). However, CBN concentrations can increase over time. In poor storage conditions, the plant’s THCA can degrade into CBNA, resulting in lower potency, aroma, and flavor. Cannabis processors may use various heating/extraction measures in a vacuum oven or chemical solvents to oxidize THC into CBN. This distinctive minor cannabinoid can offer many benefits for recreational, as well as medical users who make claim to being Very Effective for sleep.
When taken alone, this cannabis compound does not produce a high like THC. So let’s take a look at this in simple terms. In the human body our endocannabinoid systems (ECS), CBN has a low binding affinity with CB1 receptors BUT has a strong affinity with CB2 receptors, although it is still less than the THC. CBN appears to have similar properties as popular cannabinoids like CBD and THC.
Now the Health Benefits of CBN
Compared to research into other major cannabinoids like THC and CBD, CBN research is in its infancy stages. While most research into CBN is based on animal studies, researchers are beginning to uncover the potential benefits of CBN. Early research indicates that CBN may help relieve pain, insomnia, inflammation, appetite loss, and much more. CBN has many health benefits, including: Minimally psychoactive, Powerful sedative, Relieves pain, Anti-epileptic, Anti-inflammatory, Inhibits cancer cell growth, Stimulates appetite, Passes transdermal barrier ten times better than THC, Bone growth stimulation, Glaucoma treatment, Antibiotic Properties and additional scientific research is necessary to identify how this “CBN” affects the mind and body and safe ways to treat various health conditions. Simply put, CBN appears to be the cannabinoid that should not be ignored.
1. Potent Sedative –CBN is one of the most sedative cannabinoids in the cannabis plant, especially when used with THC and the myrcene terpene. Research suggests that CBN’s sedative effects can be used as a sleep aid for those who have insomnia. Not only may it help people get to sleep faster, but it may also prolong sleep time. A 5-mg dose of CBN may have the same sedative effect as 10 mg of Valium, a prescription medicine used as a sedative and for treating muscle spasms, anxiety, and alcohol withdrawal.
2. Pain Relief –Current research shows that CBN interacts with neurons involved with pain signaling and perception. These same neurons are affected by capsaicin, an active compound of chili peppers, known for its burning sensation. Capsaicin can be found in topicals and pain relievers. Essentially, CBN may be used to reduce pain.
3. Antibiotic –Studies have shown that CBN and other cannabinoids may be effective in treating MRSA, an infection caused by a type of staph bacteria. This strain of bacteria is becoming increasingly resistant to antibiotics. More research into CBN’s antimicrobial properties may help fight against antibiotic resistance.
4. Anti-Convulsant – THC and CBD products are powerful options in anti-convulsant treatment. CBN is also showing promise as a powerful anti-convulsant. A study on mice found that CBN has strong anti-convulsant properties, especially when used with other cannabinoids. If CBN continues to display anti-convulsive properties for muscle contractions, it may be a promising cannabinoid for patients with epilepsy.
5. Anti-Inflammatory – Cannabinoids can be used for inflammatory conditions such as rheumatoid arthritis and Crohn’s disease. While many cannabinoids have shown positive effects on inflammatory diseases, CBN is another alternative treatment option for those with inflammation. A study on mice found that CBN decreased allergen-induced mucus production.
6. Appetite Stimulant – Appetite loss can be caused by various psychological causes or medical conditions. While certain cannabinoids like CBD can suppress appetite, CBN may stimulate appetite. CBN may be helpful for cancer patients, for example, who may suffer from appetite loss due to cancer treatment.
7. Anti-Cancer – Early research shows that CBN can inhibit and stop cancer cell growth. In one type of lung cancer, CBN and other cannabinoids were found to actually reduce tumor size. While CBN has displayed therapeutic effects in cancer treatment, there is no definitive research showing CBN can manage the disease.
8. Glaucoma Relief – Early research suggests that high doses of CBN may help relieve intraocular pressure, a critical risk factor for glaucoma. CBN also has neuroprotective characteristics that may keep neurons in the back of the eye healthy. This is crazy but there are “Eye Drop Formulations” featuring CBN currently under development for glaucoma therapy.
9. Bone and Skin Health – CBN may have powerful protective properties to aid in bone health. CBN has been shown to activate stem cells in bones to create new bone cells. CBN may also be helpful in bone loss reduction, as a treatment for osteoporosis, and the promotion of bone healing. And in terms of skin health, CBN has been shown to reduce skin cell overgrowth. Topical CBN treatment may have promising effects in psoriasis treatment. In addition, CBN is much more permeable across the transdermal barrier than THC.
10. Neuroprotective – CBN has been shown to have neuroprotective qualities. In a study on animal models, researchers found that CBN showed positive effects when treating subjects with amyotrophic lateral sclerosis (ALS). CBN was shown to delay the onset of ALS. While more research needs to be done on humans, CBN shows promise as a therapeutic tool for neurodegenerative diseases.
FAQs About CBN
Can CBN Get You High? In small doses, CBN does not produce intoxicating effects. Is CBN Legal? While CBN is not explicitly listed under the Controlled Substances Act (CSA), CBN is still Schedule I substance derived from the Cannabis Plant Federally. The CSA defines cannabis as any part of the plant, except for stalks and nonviable seeds. CBN derived from hemp falls in a legal gray area. In some states, hemp-derived CBN products may be legal if they have under 0.3% THC. Every state has different rules and regulations on hemp-derived CBN and other THC analogs.
What Are High-CBN Strains? Currently, there are not many high-CBN strains compared to THC and CBD-rich varieties. Most strains have under 1% CBN. Here are a few strains that have slightly over 0.3% CBN. (Lemon Kush, Durban Poison, Blackberry, Bubble Gum, Purple Cadillac and Super Green Crack (What names lol)
Can You Buy CBN Online? In legal cannabis markets, CBN products can be purchased from licensed retailers. Hemp-derived CBN products are available from online retailers. Before buying CBN products, ensure they are lab-tested for purity and potency.
Final Thoughts on the Health Benefits of CBN – While THC and CBD may be the primary targets for research, CBN research is in its early stages and is slowly showcasing the health benefits of CBN. As a result, CBN is showing great promise for medical and recreational users and is being introduced into various products, including edibles and topicals.
New cannabis research found that a cannabis-based drug was able to kill pancreatic cancer cells. This cannabis-based drug, or rather miraculous medication, is a botanical combination of extracts from the Cyathus striatus fungus and cannabis. This powerful combo was even able to destroy all of the cancer cells without damaging any healthy cells, unlike conventional cancer treatments.
What Is Cyathus striatus Fungus?
Cyathus striatus fungus is otherwise known as a fluted bird’s nest as a result of being a “group of gasteromycetes group of mushrooms named for their similarity in shape to small bird’s nests.” These fungi are generally considered to be inedible but not poisonous “due to their tiny size,” which is also why they are easy to miss in nature.
Researchers Waill Elkhateeb and Ghoson Daba explain that this group of mushrooms has been able to “produce many novel and potent secondary metabolites that exerted different bioactivities especially as antimicrobial, antitumor, and anti-neuro inflammation activities.” The fungi found on Cyathus are saprophytes, microorganisms that live on dead organic matter. They are most commonly seen during autumn but can also be found year-round in damp and shady locations.
In their study on bird’s nest fungi, Elkhateeb and Daba explain that the “anti-inflammatory, antimicrobial and antitumor compounds isolated from these mushrooms belong to different chemical classes including steroids, terpenes, polysaccharides, fatty acids, phenolic acids and other metabolites.” However, much like cannabis, they concluded that information on these mushrooms is still unclear and that further research and investigation are needed.
Cyathus and Cannabinoids: The Cancer-Cell-Killing Duo
The treatment was developed by the biomedical company known as Cannabotech, while the study was led by Professor Faud Fares (a senior cancer researcher at the University of Haifa). The fungus was used based on the fact that it has been the subject of eight years of testing for anti-cancer properties, during which it demonstrated to have better anti-cancer results than most other fungi that were being tested.
According to PR Newswire, which reported the news from Cannabotech, the researchers made use of a cell model in order to experiment with their killer combo in order to see if it had any desirable effects on cancer cells—which it did. The cannabinoid and fungus extract duo was able to eliminate 100% of the pancreatic cancer cells in the model and it did so without damaging normal cells.
Since the Cyathus striatus fungus demonstrated better anti-cancer properties in comparison to other fungi, Fares was able to secure global and exclusive rights to use for patents he created. The professor began leading the study in an “accelerated process of developing a botanical drug as defined by the FDA.”
Cannabotech reported that the first milestone in the botanical drug development process was “defined as the adaptation of fungal growth and extraction methods to the FDA protocol for botanical drug development, which the company expects to be significantly cheaper and shorter than the development process of a standard ethical drug.” Then, the combination of the cannabinoid and fungal extract composition was examined.
The researchers were pleased to report that their cell model trial with the adapted extract was able to demonstrate five times higher anti-cancer efficacy than their original extract on top of “causing 100% mortality of pancreatic cancer cells.” They reported that they observed no damage to healthy cells in the model and that the cannabinoid extract was responsible for an 80% mortality of pancreatic cancer cells.
The team plans to complete the feasibility part of the study within 12 months (by mid-2023) and will then work with a large pharmaceutical company for its development. As part of their next milestone, the team plans to test both “the active mechanism of killing cancer cells by extracts and the combined anti-cancer efficacy of the fungus and cannabinoids together, in cells and animals.” The development of this revolutionary drug will be accompanied by Dr. Yitzhak Angel, who is a pharmacologist specializing in drug development with more than 35 years of experience.
The Stakes Are High
There are many types of fatal cancers, but pancreatic cancer is one of the most aggressive, with a very low survival rate- contributing to very high rates of mortality. So having a potential treatment for this cancer creates heaps of possibilities for other forms too. Fares stated:
“I am happy that the collaboration with Cannabotech is bearing fruit and achieving very impressive results to strengthen the research we conducted at the University of Haifa in recent years. The fact that such impressive results have been obtained in cells that mimic a subtype of pancreatic cancer that is known to be highly aggressive, reinforces the assessment that anti-cancer activity will be effective in other subtypes of pancreatic cancer as well.”
Angel, the pharmacologist consultant for Cannabotech, stated that “developing a botanical drug is a challenging process and the results we have achieved are a real indication that the extracts are effective and safe to use as an anti-cancer treatment for pancreatic cancer. We still have a way to go to substantiate that expectation, but we have good hopes to deliver real news to patients and develop a concrete solution to one of the most aggressive cancers.”
Considering the number of lives claimed by cancer and the amount of cancer-causing risks that surround us each day, research like this provides hope and comfort for those with cancer as well as those who are at high risk of developing cancer. Not only is this potential cannabis cure botanical, but it is also shaping up to be a safer and less risky treatment—which is important considering the harsh side effects associated with current cancer treatments.
Samuel Smiles, a cancer patient, stated, “Hope is like the sun, which, as we journey toward it, casts the shadow of our burden behind it”—and this research is hope.
Despite popular stereotypes, cannabis users are just as motivated as non-cannabis users.
The stereotype of the lazy stoner is a common one. It brings up images of The Dude in The Big Lebowski or a teenager next to a bong covered in snacks.
These images have plagued cannabis users but researchers at UCL, the University of Cambridge and the Institute of Psychiatry, Psychology & Neuroscience at King’s College London, have disproved this stereotype in a new study. The results show, despite popular conceptions, that regular cannabis users are just as motivated and capable of having feelings of pleasure or reward.
While our bodies can’t live forever, we can certainly work to push the boundaries of a commonly expected physical life span from seventy or seventy-five to exceed a century. And I’m not just talking about just living longer while being frail, fragile, or decrepit, but being healthy, full of life, having resilience, richness of experience, wisdom, and high level of energy. With a better understanding of the aging process and the rapidly growing scientific knowledge on how to reverse it, we now have options, our parents could have only dreamed about. And, as you will see, inducing carefully crafted changes in the endocannabinoid system (ECS), with or without the use of cannabis-based therapeutics, may turn out to play a significant role in these novel life-extension modalities. Before we dive and begin to explore what these new pathways to longevity might be it may be helpful to take a brief look at both the science of gerontology–the study of aging, and a relative newcomer to the healing arts–the cannabinoid health sciences.
Gerontology–The Science of Aging
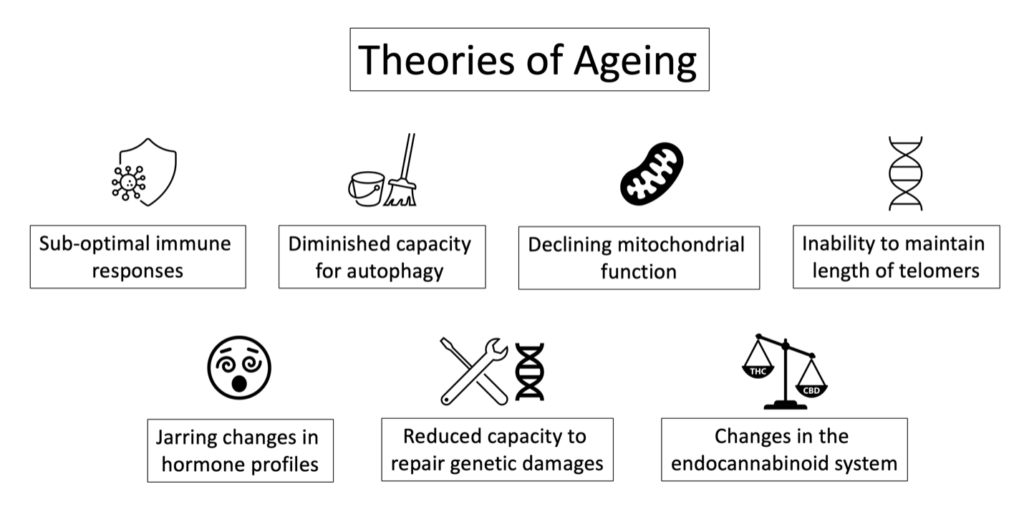
With all our technological advances it may come as a surprise that scientists do not yet have a thorough understanding of the psycho-physiological mechanism of aging. Various theories have been proposed to explain the loss of cellular integrity that we recognize as aging (see signs and symptoms below). Such theories largely focus on ineffectual immune responses after exposure to parasites, fungi, bacteria, viruses, or other pathogens; dysfunctional autophagy (allowing for the accumulation of older or damaged cells); mitochondrial dysfunction [i.e., the energy producing organelle that drives cellular energy levels and resulting (in)activity]; chronic or acute mental-emotional stress, physiological stressors such as the accumulation of toxins, the long-term effect of ionizing radiation, damage from exposure to free radicals (oxidative stressors); changes in hormone profiles; shortening of the end strings of DNA (i.e., telomeres, which occurs with each cell division and in the presence of stressors); and changes within the ECS1.
Graphic: Theories of Aging
With these changes we begin to experience suboptimal function at the level of the individual cell as well as the whole organism. In the case of the individual cell the mitochondria, begins to show degrees of dysfunction, resulting in a reduction in cellular energy production, an increase in mitochondrial waste (i.e., mitochondrial toxicity), loss of mitochondrial homeostasis, homeostatic dysfunctions, reduced capacity to protect against oxidative stress, and oxidative damage for instance. If not corrected this dysfunction can become a driver making us vulnerable to develop a great variety of chronic conditions such as neurological disease, immune disorders, cardio-vascular illness, and of course aging. The whole body now begins to manifest aging-related signs and symptoms.
Conversely, looking at life extension or longevity there are several methods or processes that have been posited to be able to extend life at the level of the individual cell and for the whole organism. Here in this article, we center our focus on ECS-based effects associated with the prevention and/or reversal of cognitive decline (e.g., dementia), facilitation of molecular clearance (i.e., optimization of autophagy e.g., Alzheimer’s disease), homeostatic defense activities, protection against neurodegeneration and/or neuro-inflammation (incl. neurogenesis), mitigation of oxidative stress, SIRT activation (a signaling protein with high potential for life extension), caloric restrictions (metabolism of fat cells is modulated by the ECS), mind-body approaches (stress is modulated by the ECS), and other therapeutic effects induced via the endocannabinoidome (the larger internal environment that interacts with the ECS).
The Cannabinoid Health Sciences (Endocannabinology)–
The Study of the Endocannabinoid System and Cannabinoid-based Therapeutics
The cannabinoid health sciences focus on the study of the endocannabinoid system (ECS). Fact is that all mammals—and that includes us humans—have a naturally occurring ECS.
The ECS is composed of receiving elements (cellular receptor sites i.e., CB1, CB2), their corresponding signaling components (i.e., endocannabinoids anandamide and 2-AG), and their essential building and degrading constituents (e.g., enzymes FAAH, MAGL). And while the ECS has been with us since time immemorial playing an essential role in maintaining our health and well-being, modern medicine discovered its existence and perhaps more importantly its vast therapeutic potential only in the late 1980’s. In fact, the first evidence of the existence of a mammalian receptor that binds with cannabinoids and cannabis-based constituents was discovered in the brains of rats (1988) when government researchers from the National Institutes of Mental Health (Bethesda) characterized a cannabinoid receptor that a few years later would be classified as cannabinoid receptor 1 (CB1).1 A few years later researchers from Cambridge University discovered the second later to be identified as CB2.2
Since then, the number of annual studies published in the attempt to understand and utilize the ECS in the potential treatment of more than 250 conditions has grown considerably. By 2022 an average of about 10 new studies have been published daily, signaling the excitement in the medical research community eager to make a difference in the lives of many chronic patient populations including those affected by signs and symptoms of aging.
Signs and Symptoms of Aging
Physical signs and symptoms: Wrinkles, “age spots,” greying hair, loss of muscle mass, loss of height, weight gain (associated with metabolic syndrome, insulin resistance, diabetes), loss of visual focus, loss of energy (i.e., at the level of the cell and the whole body), longer recovery times, male/female menopause, epigenetic changes, mutation, telomere shortening, loss of genetic stability and DNA repair capacities, loss of optimal organ/system functions, dysfunctional autophagy, mitochondrial dysfunction, dysfunction of the ECS, increased vulnerability to develop chronic degenerative illness associated with aging such as cancer, cardiovascular diseases, osteoporosis, and obesity for example.
Mental-emotional signs and symptoms of sub-optimal aging: may include cognitive decline or dysfunction (e.g., on a spectrum between forgetfulness–dementia), social isolation (e.g., loneliness, hopelessness), mood disorders (e.g., depression, anxiety, rapid fluctuations in mood), ruminating (esp. at night), lack of mental-emotional energy and/or focus, loss of social skills and/or functions.
The Endocannabinoid System and Aging in General
Over the past three decades the therapeutic potential of modulating the ECS for the treatment of aging and age-related human pathologies has gained momentum and significant interest, especially in the areas of cognitive decline (e.g., dementia, Alzheimer’s disease), facilitation of molecular clearance, homeostatic defense activities, neurodegeneration and/or inflammation, neurogenesis, and oxidative stress. Optimal function or dysfunction of the ECS such as modulation of the classical endocannabinoid receptor sites CB1 and CB2, or other cannabinoid sensitive receptor sites such as TRPV-1 may play a significant role in how we age.
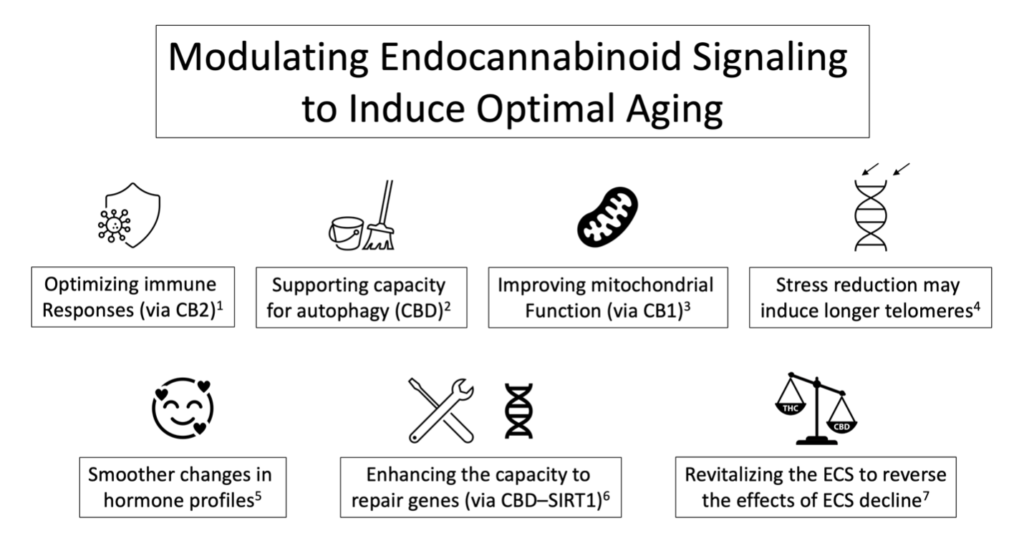
More specifically, the capacity of the body to produce endocannabinoids, to metabolize them, as well as actual endocannabinoid receptor expression and with it optimal ECS-based signaling can change significantly as we age. You may ask why is that important? For example, a reduction in endocannabinoid receptor sites has been associated with accelerated aging. Therefore, the targeted use of cannabis-based therapeutics to support optimal ECS function and with it, optimal homeostatic responses, may mitigate several of the underlying pathologies associated with the aging process. Consider these recent discoveries highlighting several emerging insights with potential clinical applications that allow us to make informed decisions about the use of cannabis-based therapeutics to shift the typically pathological aging process to one of optimal aging:
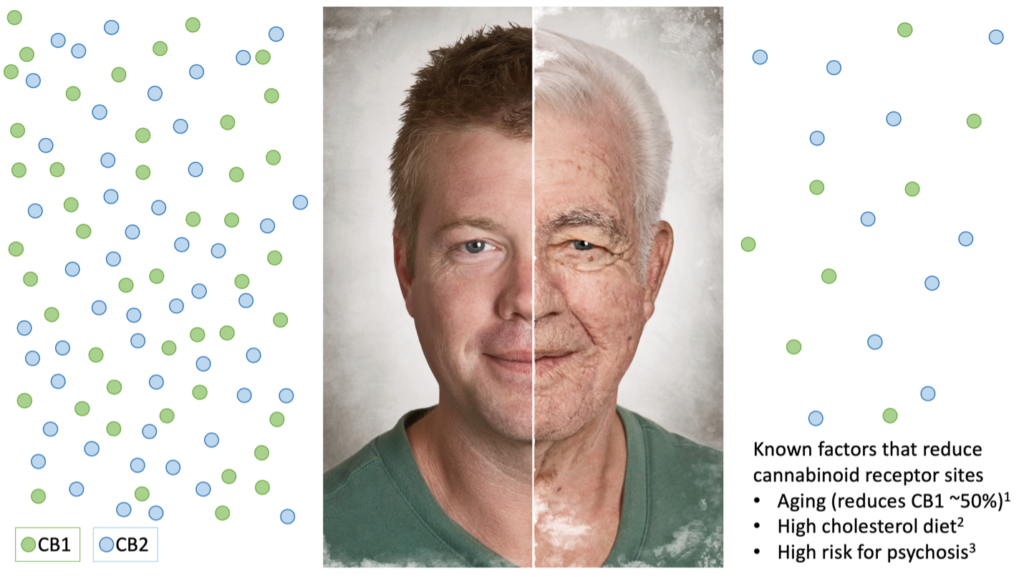
Graphic: Young/Old Man’s Face
Expression of cannabinoid receptor sites and cannabinoid signaling changes as we age.1 More specifically, CB1 expression decreases by ~50% over a human life span,2 which impairs neuronal network integrity and cognitive functions.3
Rodents bred without CB1 receptor sites show signs of accelerated aging in the brain and skin.4
The ECS supports neuroprotection, is neuro-supportive, reduces oxidative stress, stabilize glial activity, mitigates glutamate excitotoxicity, aids in metabolic homeostasis, and autophagy, all of which are associated with aging.5
Decline of ECS-based signaling on GABAergic neurons may lead to accelerated brain aging.6
Deletion of CB2 leads to severe osteoporosis in the test animals indicating a significant role of CB2 in maintaining healthy bone structures in aging mammals.7
Enhancing CB18 and CB29 signaling enhances neurogenesis, reduces neuronal decline, and reduce the ill-effects of pathological aging upon neuroinflammation.10
Cannabinoids and melatonin induce therapeutic effects fundamentally related to its anti-inflammatory and antioxidative actions at the mitochondrial level.11
CB1 activity in the mitochondria declines with age and is associated with signs of aging such as impaired memory for example. ECS-based activity may counteract the progression of brain aging.12
CBD exposure to zebrafish in utero increased longevity by about 20% (in females), reduced inflammation and decreased sperm production.13
Only lower doses of THC increased longevity, significantly reduced weight, inflammation, and reduced several senescence markers in male zebrafish.14
Cannabis-based therapeutics may be effective in the treatment of nighttime agitation,15 disinhibition, irritability, and aberrant motor behavior commonly associated with dementia.16
A chronic low dose of Δ9-tetrahydrocannabinol (THC) restores cognitive function in old mice.17
The ECS may protect against aging via homeostatic defense systems such as its antioxidant effects, facilitation of clearance, anti-inflammatory effects, and initiating neuroprotection.18
The ECS is intricately involved in the process of central and peripheral cells.19
Beta-Caryophyllene, a cannabis-common terpene and FDA approved food additive binds with CB2 and protects against cognitive impairment caused by neuro-inflammation.20
A high cholesterol diet reduces the amount of CB1 receptor sites.21
A growing body of the scientific literature clearly implicates the ECS in modulating mitochondrial function22 and as such may play a significant role in several chronic pathologies including the aging process.
More specifically, CB1 receptors have been located at the membranes of neuronal23 and muscle24 mitochondria controlling cellular respiration and energy production with potential relevance to the aging process.
Similarly, FAAH the enzyme that metabolizes AEA appears to be located on the membrane of the mitochondria and as such may play a role in the aging process.25
CBD may reverse mitochondrial dysfunction via restoring Ca2+ homeostasis.26
Stress reduction techniques may halt telomere shortening or even extend them. As such cannabis, famous for its capacity to induce deep relaxation, may turn out to play a significant role in mitigating telomere-associated cellular senescence.27
Anandamide-induced may be a therapeutic strategy in estrogen-deficient conditions (via upregulation of heme oxygenase (HO) and nitric oxide synthase (NOS) enzymes with potential relevance to menopause.28
After this summary about the ECS and aging in general let us now look at some of the latest research findings involving sirtuins.
Graphic: Modulating Endocannabinoid Signaling to Induce Optimal Aging
SIRT1– Novel Pathways to Longevity
Sirtuins–what are they and what role do they play in life extension or anti-aging? Sirtuins are signaling proteins found in all domains of life. In humans a family of seven have been identified (i.e., produced by the genes SIRT 1-7) and to-date SIRT1 has emerged as the one most studied and with the highest potential for life extension.1 Some of the most important effects of SIRT1 in the context of longevity lies in the observations that:
SIRT1 may prevent age-related diseases and support healthy aging by protecting telomere integrity.2
Initiate the repair of damaged DNA (via the activation of repair proteins).3
Generate and maintain cellular integrity and health by inducing optimal epigenetic expressions (i.e., by turning on healthy genes and by turning off unhealthy ones).4
Reduces cellular energy stress during aging and age-related diseases.5
Optimize cellular function.6
Optimize cellular metabolism with relevance to age-related metabolic syndrome, obesity, diabetes, and age-related liver dysfunction (by producing a metabolic shift away from carbohydrates to the use of fat).7
Mitigate oxidative stress.8
Detoxification or clearance of old and dying cells (i.e., autophagy) thus support cellular renewal.9
Reduces mitochondrial damage and death and promotes energy metabolism.10
Similarly, to several components of the ECS, SIRT1 expression and activity too decreases with sub-optimal aging and in the presence of chronic stressors such as age-related diseases.11
Homeostatic maintenance and with it the regulation of lifespan involves SIRT1 via the hypothalamus-pituitary axis.13
Graphic: Modulating SIRT1 Signaling to Induce Optimal Aging
The Endocannabinoid System and SIRT1–Research Findings with Potential Clinical Relevance
Up to this point we explored the roles the ECS and SIRT1 play individually in mitigating the signs and symptoms of pathological aging. Now, we are ready to look at novel research results that offer additional and surprising insights. As it turns out, the reason why modulating components of the ECS with cannabis-based therapeutics (e.g., CBD) work to mitigate sub-optimal aging and as such work toward realizing longevity is at least in part due to their ability to support and harness the anti-aging effects initiated by healthy SIRT1 expressions. Consider these preclinical key findings:
A team of researchers from the Kunming Medical University and Hospital of People’s Liberation Army, Kaiyuan, China (2021) discovered that CBD extends the lifespan and rescues age-associated physiological declines. CBD induced autophagy and protects nerve cells from mitochondrial dysfunction via modulation of SIRT1.1
A multi-institutional team of Australian scientists including the Australian Centre for Cannabinoid Clinical and Research Excellence (2022) learned that upregulation in the expression of SIRT1 via the use of CBD resulted in enhanced longevity and neuroprotection.2
A US-based team from the National Institutes of Health, Bethesda, MD (2020) reported that antagonism at CB1 improves hepatic insulin signaling and glycemic control in obese mice via activation of SIRT1 (mTORC2/Akt pathway). To provide the reader with some practical context, the cannabis constituent THCV is a known antagonist at CB1.3
Another group of researchers from the Nanjing Medical University in China (2013) found additional insights implicating CB2. More specifically, agonism at CB2 induced fatty acid oxidation via SIRT1 activation and thus may be a future target in the treatment of conditions that share an underlying pathology of lipid dysregulation.4 To provide the reader with some practical context, THC, or the cannabis-common terpene beta-caryophyllene are known agonist at CB2.
As you can see, CBD is emerging as a significant cannabinoid of interest. Future research will undoubtedly explore any potential effects (e.g., agonism vs antagonism) cannabinoids (or other cannabis-constituents) can induce via activation of CB1, CB2, other receptor sites or via the modulating of components of the endocannabinoidome (see next paragraph).
SIRT1 and the Endocannabinoidome
Curcumin
Curcumin is readily available and potent biologically active compound found in turmeric. Curcumin induces SIRT1 upregulation may be beneficial against several age-related conditions such as metabolic syndrome, obesity, and diabetes.1 It is also part of the larger endocannabinoidome i.e., the physiological environment that is responsive to changes in the ECS. For instance, while turmeric it does not bind with CB1 or CB2 it affects their actual numbers (expression) and as such may be quite able to modulate all the effects associated with these receptor sites.2 Emerging research findings suggest potentially significant value for patients manifesting age-related signs in the form of heart disease3 (e.g. angina, heart attack, reperfusion injuries), Alzheimer’s disease (e.g., neuroprotective, anti-inflammatory, antioxidant, improved mitochondrial functions),4 or the aging of cells that make up the lining of blood vessels and lymphatic vessels.5
Omega-3
The lipidome is a full accounting of all lipids embedded in the membranes of each individual cell. Lipids are a family of naturally occurring compounds that together build much of the internal architecture of living cells. Cellular membranes can be thought of as the skin of the cell. The skin of our trillions of individual cells is made from lipids containing a vast number of lipophilic (“fat-loving”) receptor sites such as CB1 or CB2 for example ready to interact with lipophilic compounds such as cannabinoids. Polyunsaturated fatty acids (PUFAs) are essential building blocks. Since the human body does not make its own PUFAs, we must consume them to survive and thrive. PUFAs such as omega-3 and omega-6 fatty acids are primary building blocks the body uses to make its own endocannabinoids. And here is an important insight: a healthy ECS is dependent on the ratio of omega-3 to omega-6. Excess of omega-6 and a lack of dietary omega-3 are implicated in a poorly functioning ECS.6 And, if you need another reason to motivate yourself to eat healthy fat consider that a high cholesterol diet reduces the amount of available CB1 receptor sites and with it all the potentially beneficial effects associated with them.7
Caloric Restriction
It has been posited that caloric restriction improves longevity and mitigates the development of age-related disorders (e.g., cancer)8 via several mechanism aimed at the contributing pathologies of aging including the clearance of accumulating aging and damaged cells (i.e., autophagy), improving mitochondrial energy production, and inducing antioxidant effects, for example. It is inexpensive, everyone can do it, and all is needed is the decision and the will to see it through. The good news for those of us who have a more difficult time with sticking to a diet the use of polyphenols produces similar results and as such is considered a caloric-restriction mimetic.9 Polyphenolic compounds (e.g., resveratrol, curcumin, quercetin) contained in dark grapes, turmeric, and fresh capers respectively for instance upregulate SIRT1 activity10 and as such may produce similar effects as caloric restrictions. In addition, CB1 antagonism (via a synthetic cannabinoid) has been demonstrated to create a synergy alongside caloric restriction and exercise resulting in weight-loss, improved glucose metabolism, and better cardiovascular function11 all-important markers typically used to measure signs of aging.
SIRT1 Cautions
While most of the emerging research results have explored the therapeutic potential of SIRT1 e.g., being a tumor suppressor,1 a few others have produced results that suggest that SIRT1 may act in some cases as or tumor promoter2 suggesting a more complex role (e.g., utilizing either SIRT1 agonists or antagonists) yet to be fully understood.3
In addition, overexpression of SIRT1 may induce potential adverse effects such as worsening inflammation in patients suffering from MS and autoimmune disorders such as rheumatoid arthritis.4
Furthermore, in the context of head and neck cancer SIRT1 gene silencing decreased ferroptosis (cell death induced by iron-dependent accumulation of lethal lipid peroxidation). In direct contrast, SIRT inducers such as resveratrol increased ferroptosis.5
Summary and Practical Steps to Optimize the Aging Process
While many of the longevity-related trial data is based on preclinical trials, i.e., not conducted on humans and, while much remains to be learned about how specifically cannabinoid-based therapeutics may be utilized to reach for longevity, these early findings and the potential for emerging treatment trends is already pushing the envelope of what we know about aging and the notion of life-extension itself. Here is a summary of related research findings the reader might find instructive:
Cannabidiol (CBD) is a primary cannabinoid that does not produce changes in cognition but tends to provide a gentle uplift in mood. The preclinical trials mentioned above have suggested that CBD-based modulation of various components of the ECS including that of SIRT1 may produce beneficial effects toward optimal aging.
Delta-9-tetrahydrocannabinol is the primary psychoactive compound found in cannabis. The pre-clinical trials mentioned above have suggested that small amounts of THC may be beneficial while larger amounts have produced mixed or detrimental effects. THC activates CB1 and CB2 and as such may prevent and/or mitigates cognitive decline, supports neuroprotection, anti-neuroinflammatory effects, and neurogenesis. The reader is reminded that most adverse effects associated with the use of cannabis are produced by THC in a dose-dependent fashion. In other words, the higher the mg dose of THC the higher the risk of experiencing an adverse effect. THC dosing consideration (based on usage in clinical trials):
THC microdose: 0.1 mg to 0.4 mg
THC low dose: 0.5 mg to 5 mg
THC medium dose: 6 mg to 20 mg
THC high dose: 21 mg to 50+ mg
While already stated previously but worth repeating here, the endocannabinoidome is the larger internal environment that responds to changes in the ECS that are beyond those changes initiated by the classical endocannabinoid receptor sites (i.e., CB1 and CB2). These changes may be food-dependent, based on cannabinoid-based therapeutics, or initiated via mind-body approaches (more about that in part 2). And, since their impact can significantly support a healthy aging process, we wanted to include, at least those mentioned above, here at the very end of the article.
Turmeric may increase endocannabinoid receptor site expression and as such may mitigate age-dependent loss of endocannabinoid receptor sites and signaling.
Beta-caryophyllene activates CB2 receptor sites and may mitigate are-related neuroinflammation and associated cognitive decline.
Caloric restrictions, a proven life-extension method, depends, in part, on ECS-based changes in fat cell metabolism.
Increasing omega-3 intake may make cannabinoid more bioavailable and as such may support the beneficial effects associated with them (also consider reducing omega-6 and avoid unhealthy fats e.g., trans-fats).
Reducing stress and increasing activities that induce deep relaxation is significantly modulated via the ECS (more about this in part 2).
In Part 2 we will examine the latest research results focusing on where the cannabinoid health sciences overlap with research results from the field of mind-body medicine and what practical relevance and techniques can be used to mitigate pathological aging and instead to harness optimal aging and longevity.
Endnotes: Gerontology–The Science of Aging
1. Bilkei-Gorzo A. (2012). The endocannabinoid system in normal and pathological brain ageing. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 367(1607), 3326–3341.
Endnotes: The Cannabinoid Health Sciences
1. Devane WA, Dysarz FA 3rd, Johnson MR, Melvin LS, Howlett AC (1988 Nov). Determination and characterization of a cannabinoid receptor in rat brain. Mol Pharmacol. 34(5):605-613.
2. Munro S, Thomas KL, Abu-Shaar M. (1993 Sep). Molecular characterization of a peripheral receptor for cannabinoids. Nature. 365(6441):61-5.
Endnotes: The Endocannabinoid System and Aging in General
Endnotes, graphic (Young/Old Man’s Face):
1. Kataoka K, Bilkei-Gorzo A, Nozaki C, Togo A, Nakamura K, Ohta K, Zimmer A, Asahi T. (2020 Jul) Age-dependent Alteration in Mitochondrial Dynamics and Autophagy in Hippocampal Neuron of Cannabinoid CB1 Receptor-deficient Mice. Brain Res Bull. 160:40-49.
2. Hayakawa K, Mishima K, Nozako M, Hazekawa M, Aoyama Y, Ogata A, Harada K, Fujioka M, Abe K, Egashira N, Iwasaki K, Fujiwara M. (2007 Mar) High-cholesterol feeding aggravates cerebral infarction via decreasing the CB1 receptor. Neurosci Lett. 414(2):183-7.
3. Joaquim HPG, Costa AC, Pereira CAC, Talib LL, Bilt MMV, Loch AA, Gattaz WF. Plasmatic endocannabinoids are decreased in subjects with ultra-high risk of psychosis. Eur J Neurosci. 2021 Oct 29.
Endnotes to text:
1. Bilkei-Gorzo A. (2012). The endocannabinoid system in normal and pathological brain ageing. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 367(1607), 3326–3341.
Romero J, Berrendero F, Garcia-Gil L, de la Cruz P, Ramos JA, Fernández-Ruiz JJ. (1998 Jun) Loss of cannabinoid receptor binding and messenger RNA levels and cannabinoid agonist-stimulated [35S]guanylyl-5’O-(thio)-triphosphate binding in the basal ganglia of aged rats. Neuroscience. 84(4):1075-83.
Berrendero F, Romero J, García-Gil L, Suarez I, De la Cruz P, Ramos JA, Fernández-Ruiz JJ. (1998 Sep 30) Changes in cannabinoid receptor binding and mRNA levels in several brain regions of aged rats. Biochim Biophys Acta. 1407(3):205-14.
Van Laere K, Goffin K, Casteels C, Dupont P, Mortelmans L, de Hoon J, Bormans G. Gender-dependent increases with healthy aging of the human cerebral cannabinoid-type 1 receptor binding using [(18)F]MK-9470 PET. Neuroimage. 2008 Feb 15;39(4):1533-41.
Wang, L., Liu, J., Harvey-White, J., Zimmer, A., & Kunos, G. (2003). Endocannabinoid signaling via cannabinoid receptor 1 is involved in ethanol preference and its age-dependent decline in mice. Proceedings of the National Academy of Sciences of the United States of America, 100(3), 1393–1398.
2. Long, L. E., Lind, J., Webster, M., & Weickert, C. S. (2012). Developmental trajectory of the endocannabinoid system in human dorsolateral prefrontal cortex. BMC neuroscience, 13, 87.
3. Kataoka K, Bilkei-Gorzo A, Nozaki C, Togo A, Nakamura K, Ohta K, Zimmer A, Asahi T. (2020 Jul) Age-dependent Alteration in Mitochondrial Dynamics and Autophagy in Hippocampal Neuron of Cannabinoid CB1 Receptor-deficient Mice. Brain Res Bull. 160:40-49.
4. Bilkei-Gorzo A, Drews E, Albayram Ö, Piyanova A, Gaffal E, Tueting T, Michel K, Mauer D, Maier W, Zimmer A. Early onset of aging-like changes is restricted to cognitive abilities and skin structure in Cnr1⁻/⁻ mice. Neurobiol Aging. 2012 Jan;33(1):200.e11-22.
5. Carrera, J., Tomberlin, J., Kurtz, J., Karakaya, E., Bostanciklioglu, M., & Albayram, O. (2021). Endocannabinoid Signaling for GABAergic-Microglia (Mis)Communication in the Brain Aging. Frontiers in neuroscience, 14, 606808.
6. Ibid.
7. Ofek, O., Karsak, M., Leclerc, N., Fogel, M., Frenkel, B., Wright, K., Tam, J., Attar-Namdar, M., Kram, V., Shohami, E., Mechoulam, R., Zimmer, A., & Bab, I. (2006). Peripheral cannabinoid receptor, CB2, regulates bone mass. Proceedings of the National Academy of Sciences of the United States of America, 103(3), 696–701.
8. Jiang, W., Zhang, Y., Xiao, L., Van Cleemput, J., Ji, S. P., Bai, G., & Zhang, X. (2005). Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic- and antidepressant-like effects. The Journal of clinical investigation, 115(11), 3104–3116.
9. Goncalves MB, Suetterlin P, Yip P, Molina-Holgado F, Walker DJ, Oudin MJ, Zentar MP, Pollard S, Yáñez-Muñoz RJ, Williams G, Walsh FS, Pangalos MN, Doherty P. (2008 Aug) A diacylglycerol lipase-CB2 cannabinoid pathway regulates adult subventricular zone neurogenesis in an age-dependent manner. Mol Cell Neurosci. 38(4):526-36.
10. Marchalant Y, Brothers HM, Norman GJ, Karelina K, DeVries AC, Wenk GL. Cannabinoids attenuate the effects of aging upon neuroinflammation and neurogenesis. Neurobiol Dis. 2009 May;34(2):300-7.
11. García S, Martín Giménez VM, Mocayar Marón FJ, Reiter RJ, Manucha W. (2020 Aug) Melatonin and cannabinoids: mitochondrial-targeted molecules that may reduce inflammaging in neurodegenerative diseases. Histol Histopathol. 35(8):789-800.
12. Kataoka K, Bilkei-Gorzo A, Nozaki C, Togo A, Nakamura K, Ohta K, Zimmer A, Asahi T. (2020 Jul) Age-dependent Alteration in Mitochondrial Dynamics and Autophagy in Hippocampal Neuron of Cannabinoid CB1 Receptor-deficient Mice. Brain Res Bull. 160:40-49.
13. Pandelides, Z., Thornton, C., Faruque, A. S., Whitehead, A. P., Willett, K. L., & Ashpole, N. M. (2020). Developmental exposure to cannabidiol (CBD) alters longevity and health span of zebrafish (Danio rerio). GeroScience, 42(2), 785–800.
14. Pandelides, Z., Thornton, C., Lovitt, K. G., Faruque, A. S., Whitehead, A. P., Willett, K. L., & Ashpole, N. M. (2020). Developmental exposure to Δ9-tetrahydrocannabinol (THC) causes biphasic effects on longevity, inflammation, and reproduction in aged zebrafish (Danio rerio). GeroScience, 42(3), 923–936.
15. Walther S, Mahlberg R, Eichmann U, Kunz D. (2006 May) Delta-9-tetrahydrocannabinol for nighttime agitation in severe dementia. Psychopharmacology (Berl). 185(4):524-8.
16. Medical Cannabis for the Treatment of Dementia: A Review of Clinical Effectiveness and Guidelines. Ottawa: CADTH; 2019 Jul. (Canadian Agency for Drugs and Technologies in Health rapid response report: summary with critical appraisal).
17. Bilkei-Gorzo, A., Albayram, O., Draffehn, A. et al. (2017) A chronic low dose of Δ9-tetrahydrocannabinol (THC) restores cognitive function in old mice. Nat Med 23, 782–787.
18. Bilkei-Gorzo A. (2012). The endocannabinoid system in normal and pathological brain ageing. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 367(1607), 3326–3341.
19. Paradisi A, Oddi S, Maccarrone M. (2006 Nov) The endocannabinoid system in ageing: a new target for drug development. Curr Drug Targets. 7(11):1539-52.
20. Kanojia U, Chaturbhuj SG, Sankhe R, Das M, Surubhotla R, Krishnadas N, Gourishetti K, Nayak PG, Kishore A. Beta-Caryophyllene, a CB2R Selective Agonist, Protects Against Cognitive Impairment Caused by Neuro-inflammation and Not in Dementia Due to Ageing Induced by Mitochondrial Dysfunction. CNS Neurol Disord Drug Targets. 2021;20(10):963-974.
21. Hayakawa K, Mishima K, Nozako M, Hazekawa M, Aoyama Y, Ogata A, Harada K, Fujioka M, Abe K, Egashira N, Iwasaki K, Fujiwara M. (2007 Mar) High-cholesterol feeding aggravates cerebral infarction via decreasing the CB1 receptor. Neurosci Lett. 414(2):183-7.
22. Nunn A, Guy G, Bell JD. (2012 Dec 5) Endocannabinoids in neuroendopsychology: multiphasic control of mitochondrial function. Philos Trans R Soc Lond B Biol Sci. 367(1607):3342-52.
Lipina C, Irving AJ, Hundal HS. (2014 Jul) Mitochondria: a possible nexus for the regulation of energy homeostasis by the endocannabinoid system? Am J Physiol Endocrinol Metab. 307(1):E1-13.
Fišar Z, Singh N, Hroudová J. (2014 Nov) Cannabinoid-induced changes in respiration of brain mitochondria. Toxicol Lett. 231(1):62-71.
Singh N, Hroudová J, Fišar Z. (2015 Aug) Cannabinoid-Induced Changes in the Activity of Electron Transport Chain Complexes of Brain Mitochondria. J Mol Neurosci. 56(4):926-931.
Catanzaro G, Rapino C, Oddi S, Maccarrone M. (2009 Oct 16) Anandamide increases swelling and reduces calcium sensitivity of mitochondria. Biochem Biophys Res Commun. 388(2):439-42.
Zhou S, Ling X, Meng P, Liang Y, Shen K, Wu Q, Zhang Y, Chen Q, Chen S, Liu Y, Zhou L. (2021 Sep) Cannabinoid receptor 2 plays a central role in renal tubular mitochondrial dysfunction and kidney ageing. J Cell Mol Med. 25(18):8957-8972.
Zaccagnino P, D’Oria S, Romano LL, Di Venere A, Sardanelli AM, Lorusso M. (2012 Apr) The endocannabinoid 2-arachidonoylglicerol decreases calcium induced cytochrome c release from liver mitochondria. J Bioenerg Biomembr. 44(2):273-80.
Lu Y, Lee DI, Roy Chowdhury S, Lu P, Kamboj A, Anderson CM, Fernyhough P, Anderson HD. (2020 Jan) Activation of Cannabinoid Receptors Attenuates Endothelin-1-Induced Mitochondrial Dysfunction in Rat Ventricular Myocytes. J Cardiovasc Pharmacol. 75(1):54-63.
Oláh A, Alam M, Chéret J, Kis NG, Hegyi Z, Szöllősi AG, Vidali S, Bíró T, Paus R. (. 2020 Jul) Mitochondrial energy metabolism is negatively regulated by cannabinoid receptor 1 in intact human epidermis. Exp Dermatol29(7):616-622.
23. Bénard G, Massa F, Puente N, Lourenço J, Bellocchio L, Soria-Gómez E, Matias I, Delamarre A, Metna-Laurent M, Cannich A, Hebert-Chatelain E, Mulle C, Ortega-Gutiérrez S, Martín-Fontecha M, Klugmann M, Guggenhuber S, Lutz B, Gertsch J, Chaouloff F, López-Rodríguez ML, Grandes P, Rossignol R, Marsicano G. (2012 Mar 4). Mitochondrial CB₁ receptors regulate neuronal energy metabolism. Nat Neurosci. 15(4):558-64.
Hebert-Chatelain E, Desprez T, Serrat R, Bellocchio L, Soria-Gomez E, Busquets-Garcia A, Pagano Zottola AC, Delamarre A, Cannich A, Vincent P, Varilh M, Robin LM, Terral G, García-Fernández MD, Colavita M, Mazier W, Drago F, Puente N, Reguero L, Elezgarai I, Dupuy JW, Cota D, Lopez-Rodriguez ML, Barreda-Gómez G, Massa F, Grandes P, Bénard G, Marsicano G. (2016 Nov 24) A cannabinoid link between mitochondria and memory. Nature. 539(7630):555-559.
Jimenez-Blasco D, Busquets-Garcia A, Hebert-Chatelain E, Serrat R, Vicente-Gutierrez C, Ioannidou C, Gómez-Sotres P, Lopez-Fabuel I, Resch-Beusher M, Resel E, Arnouil D, Saraswat D, Varilh M, Cannich A, Julio-Kalajzic F, Bonilla-Del Río I, Almeida A, Puente N, Achicallende S, Lopez-Rodriguez ML, Jollé C, Déglon N, Pellerin L, Josephine C, Bonvento G, Panatier A, Lutz B, Piazza PV, Guzmán M, Bellocchio L, Bouzier-Sore AK, Grandes P, Bolaños JP, Marsicano G. (2020 Jul) Glucose metabolism links astroglial mitochondria to cannabinoid effects. Nature. 583(7817):603-608.
24. Mendizabal-Zubiaga J, Melser S, Bénard G, Ramos A, Reguero L, Arrabal S, Elezgarai I, Gerrikagoitia I, Suarez J, Rodríguez De Fonseca F, Puente N, Marsicano G, Grandes P. (2016 Oct 25) Cannabinoid CB1 Receptors Are Localized in Striated Muscle Mitochondria and Regulate Mitochondrial Respiration. Front Physiol. 7:476.
25. Morozov YM, Ben-Ari Y, Freund TF. (2004 Jul) The spatial and temporal pattern of fatty acid amide hydrolase expression in rat hippocampus during postnatal development. Eur J Neurosci. 20(2):459-66.
26. Ryan D, Drysdale AJ, Lafourcade C, Pertwee RG, Platt B. (2009 Feb 18) Cannabidiol targets mitochondria to regulate intracellular Ca2+ levels. J Neurosci. 29(7):2053-63.
27. Lengacher CA, Reich RR, Kip KE, Barta M, Ramesar S, Paterson CL, Moscoso MS, Carranza I, Budhrani PH, Kim SJ, Park HY, Jacobsen PB, Schell MJ, Jim HS, Post-White J, Farias JR, Park JY. (2014 Oct) Influence of mindfulness-based stress reduction (MBSR) on telomerase activity in women with breast cancer (BC). Biol Res Nurs. 16(4):438-47.
Schutte NS, Malouff JM, Keng SL. (2020 Aug) Meditation and telomere length: a meta-analysis. Psychol Health. 35(8):901-915.
Innes KE, Selfe TK, Brundage K, Montgomery C, Wen S, Kandati S, Bowles H, Khalsa DS, Huysmans Z. (2018). Effects of Meditation and Music-Listening on Blood Biomarkers of Cellular Aging and Alzheimer’s Disease in Adults with Subjective Cognitive Decline: An Exploratory Randomized Clinical Trial. J Alzheimers Dis. 66(3):947-970.
Dasanayaka NN, Sirisena ND, Samaranayake N. (2021 May). The effects of meditation on length of telomeres in healthy individuals: a systematic review. Syst Rev. 10(1):151.
28. Szabó R, Börzsei D, Szabó Z, Hoffmann A, Zupkó I, Priksz D, Kupai K, Varga C, Pósa A. (2020 Nov) A Potential Involvement of Anandamide in the Modulation of HO/NOS Systems: Women, Menopause, and “Medical Cannabinoids”. Int J Mol Sci. 21(22):8801.
Graphic: Modulating Endocannabinoid Signaling to Induce Optimal Aging
1. Zheng X, Sun T, Wang X. Activation of type 2 cannabinoid receptors (CB2R) promotes fatty acid oxidation through the SIRT1/PGC-1α pathway. Biochem Biophys Res Commun. 2013 Jul 5;436(3):377-81.
2. Kang, S., Li, J., Yao, Z., & Liu, J. (2021). Cannabidiol Induces Autophagy to Protects Neural Cells from Mitochondrial Dysfunction by Upregulating SIRT1 to Inhibits NF-κB and NOTCH Pathways. Frontiers in cellular neuroscience, 15, 654340.
Wang, Z., Zheng, P., Chen, X. et al. Cannabidiol induces autophagy and improves neuronal health associated with SIRT1 mediated longevity. GeroScience (2022).
3. García S, Martín Giménez VM, Mocayar Marón FJ, Reiter RJ, Manucha W. (2020 Aug) Melatonin and cannabinoids: mitochondrial-targeted molecules that may reduce inflammation in neurodegenerative diseases. Histol Histopathol. 35(8):789-800.
Bénard G, Massa F, Puente N, Lourenço J, Bellocchio L, Soria-Gómez E, Matias I, Delamarre A, Metna-Laurent M, Cannich A, Hebert-Chatelain E, Mulle C, Ortega-Gutiérrez S, Martín-Fontecha M, Klugmann M, Guggenhuber S, Lutz B, Gertsch J, Chaouloff F, López-Rodríguez ML, Grandes P, Rossignol R, Marsicano G. (2012 Mar 4). Mitochondrial CB₁ receptors regulate neuronal energy metabolism. Nat Neurosci. 15(4):558-64.
Hebert-Chatelain E, Desprez T, Serrat R, Bellocchio L, Soria-Gomez E, Busquets-Garcia A, Pagano Zottola AC, Delamarre A, Cannich A, Vincent P, Varilh M, Robin LM, Terral G, García-Fernández MD, Colavita M, Mazier W, Drago F, Puente N, Reguero L, Elezgarai I, Dupuy JW, Cota D, Lopez-Rodriguez ML, Barreda-Gómez G, Massa F, Grandes P, Bénard G, Marsicano G. (2016 Nov 24) A cannabinoid link between mitochondria and memory. Nature. 539(7630):555-559.
Jimenez-Blasco D, Busquets-Garcia A, Hebert-Chatelain E, Serrat R, Vicente-Gutierrez C, Ioannidou C, Gómez-Sotres P, Lopez-Fabuel I, Resch-Beusher M, Resel E, Arnouil D, Saraswat D, Varilh M, Cannich A, Julio-Kalajzic F, Bonilla-Del Río I, Almeida A, Puente N, Achicallende S, Lopez-Rodriguez ML, Jollé C, Déglon N, Pellerin L, Josephine C, Bonvento G, Panatier A, Lutz B, Piazza PV, Guzmán M, Bellocchio L, Bouzier-Sore AK, Grandes P, Bolaños JP, Marsicano G. (2020 Jul) Glucose metabolism links astroglial mitochondria to cannabinoid effects. Nature. 583(7817):603-608.
Mendizabal-Zubiaga J, Melser S, Bénard G, Ramos A, Reguero L, Arrabal S, Elezgarai I, Gerrikagoitia I, Suarez J, Rodríguez De Fonseca F, Puente N, Marsicano G, Grandes P. (2016 Oct 25) Cannabinoid CB1 Receptors Are Localized in Striated Muscle Mitochondria and Regulate Mitochondrial Respiration. Front Physiol. 7:476.
4. Lengacher CA, Reich RR, Kip KE, Barta M, Ramesar S, Paterson CL, Moscoso MS, Carranza I, Budhrani PH, Kim SJ, Park HY, Jacobsen PB, Schell MJ, Jim HS, Post-White J, Farias JR, Park JY. (2014 Oct) Influence of mindfulness-based stress reduction (MBSR) on telomerase activity in women with breast cancer (BC). Biol Res Nurs. 16(4):438-47.
Schutte NS, Malouff JM, Keng SL. (2020 Aug) Meditation and telomere length: a meta-analysis. Psychol Health. 35(8):901-915.
Innes KE, Selfe TK, Brundage K, Montgomery C, Wen S, Kandati S, Bowles H, Khalsa DS, Huysmans Z. (2018). Effects of Meditation and Music-Listening on Blood Biomarkers of Cellular Aging and Alzheimer’s Disease in Adults with Subjective Cognitive Decline: An Exploratory Randomized Clinical Trial. J Alzheimers Dis. 66(3):947-970.
Dasanayaka NN, Sirisena ND, Samaranayake N. (2021 May). The effects of meditation on length of telomeres in healthy individuals: a systematic review. Syst Rev. 10(1):151.
5. Szabó R, Börzsei D, Szabó Z, Hoffmann A, Zupkó I, Priksz D, Kupai K, Varga C, Pósa A. (2020 Nov 20) A Potential Involvement of Anandamide in the Modulation of HO/NOS Systems: Women, Menopause, and “Medical Cannabinoids”. Int J Mol Sci. 21(22):8801.
6. Pandelides, Z., Thornton, C., Faruque, A. S., Whitehead, A. P., Willett, K. L., & Ashpole, N. M. (2020). Developmental exposure to cannabidiol (CBD) alters longevity and health span of zebrafish (Danio rerio). GeroScience, 42(2), 785–800.
Kang, S., Li, J., Yao, Z., & Liu, J. (2021). Cannabidiol Induces Autophagy to Protects Neural Cells from Mitochondrial Dysfunction by Upregulating SIRT1 to Inhibits NF-κB and NOTCH Pathways. Frontiers in cellular neuroscience, 15, 654340.
Wang, Z., Zheng, P., Chen, X. et al. Cannabidiol induces autophagy and improves neuronal health associated with SIRT1 mediated longevity. GeroScience (2022).
7. See 1-6 above.
Endnotes: SIRT1– Novel Pathways to Longevity
1. Grabowska, W., Sikora, E., & Bielak-Zmijewska, A. (2017). Sirtuins, a promising target in slowing down the ageing process. Biogerontology, 18(4), 447–476.
2. Osum M, Serakinci N. Impact of circadian disruption on health; SIRT1 and Telomeres. DNA Repair (Amst). 2020 Dec;96:102993.
3. Oberdoerffer, P., Michan, S., McVay, M., Mostoslavsky, R., Vann, J., Park, S. K., Hartlerode, A., Stegmuller, J., Hafner, A., Loerch, P., Wright, S. M., Mills, K. D., Bonni, A., Yankner, B. A., Scully, R., Prolla, T. A., Alt, F. W., & Sinclair, D. A. (2008). SIRT1 redistribution on chromatin promotes genomic stability but alters gene expression during aging. Cell, 135(5), 907–918.
Ming, M., Shea, C. R., Guo, X., Li, X., Soltani, K., Han, W., & He, Y. Y. (2010). Regulation of global genome nucleotide excision repair by SIRT1 through xeroderma pigmentosum C. Proceedings of the National Academy of Sciences of the United States of America, 107(52), 22623–22628.
Wang, R. H., Sengupta, K., Li, C., Kim, H. S., Cao, L., Xiao, C., Kim, S., Xu, X., Zheng, Y., Chilton, B., Jia, R., Zheng, Z. M., Appella, E., Wang, X. W., Ried, T., & Deng, C. X. (2008). Impaired DNA damage response, genome instability, and tumorigenesis in SIRT1 mutant mice. Cancer cell, 14(4), 312–323.
Chung, S., Yao, H., Caito, S., Hwang, J. W., Arunachalam, G., & Rahman, I. (2010). Regulation of SIRT1 in cellular functions: role of polyphenols. Archives of biochemistry and biophysics, 501(1), 79–90.
4. Zhou CH, Zhang MX, Zhou SS, Li H, Gao J, Du L, Yin XX. SIRT1 attenuates neuropathic pain by epigenetic regulation of mGluR1/5 expressions in type 2 diabetic rats. Pain. 2017 Jan;158(1):130-139.
5. Fang, Y., Wang, X., Yang, D., Lu, Y., Wei, G., Yu, W., Liu, X., Zheng, Q., Ying, J., & Hua, F. (2021). Relieving Cellular Energy Stress in Aging, Neurodegenerative, and Metabolic Diseases, SIRT1 as a Therapeutic and Promising Node. Frontiers in aging neuroscience, 13, 738686.
6. Chung, S., Yao, H., Caito, S., Hwang, J. W., Arunachalam, G., & Rahman, I. (2010). Regulation of SIRT1 in cellular functions: role of polyphenols. Archives of biochemistry and biophysics, 501(1), 79–90.
7. Sasaki T. (2015). Age-Associated Weight Gain, Leptin, and SIRT1: A Possible Role for Hypothalamic SIRT1 in the Prevention of Weight Gain and Aging through Modulation of Leptin Sensitivity. Frontiers in endocrinology, 6, 109.
Milne, J. C., Lambert, P. D., Schenk, S., Carney, D. P., Smith, J. J., Gagne, D. J., Jin, L., Boss, O., Perni, R. B., Vu, C. B., Bemis, J. E., Xie, R., Disch, J. S., Ng, P. Y., Nunes, J. J., Lynch, A. V., Yang, H., Galonek, H., Israelian, K., Choy, W., … Westphal, C. H. (2007). Small molecule activators of SIRT1 as therapeutics for the treatment of type 2 diabetes. Nature, 450(7170), 712–716.
Jin, J., Iakova, P., Jiang, Y., Medrano, E. E., & Timchenko, N. A. (2011). The reduction of SIRT1 in livers of old mice leads to impaired body homeostasis and to inhibition of liver proliferation. Hepatology (Baltimore, Md.), 54(3), 989–998.
Li Z, Zhang Z, Ke L, Sun Y, Li W, Feng X, Zhu W, Chen S. (2020 Mar) Resveratrol promotes white adipocytes browning and improves metabolic disorders in Sirt1-dependent manner in mice. FASEB J. 34(3):4527-4539.
Timmers, S., Konings, E., Bilet, L., Houtkooper, R. H., van de Weijer, T., Goossens, G. H., Hoeks, J., van der Krieken, S., Ryu, D., Kersten, S., Moonen-Kornips, E., Hesselink, M., Kunz, I., Schrauwen-Hinderling, V. B., Blaak, E., Auwerx, J., & Schrauwen, P. (2011). Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell metabolism, 14(5), 612–622.
8. Guarente L. Sirtuins in aging and disease. Cold Spring Harb Symp Quant Biol. 2007;72:483-8.
9. Lee, I. H., Cao, L., Mostoslavsky, R., Lombard, D. B., Liu, J., Bruns, N. E., Tsokos, M., Alt, F. W., & Finkel, T. (2008). A role for the NAD-dependent deacetylase Sirt1 in the regulation of autophagy. Proceedings of the National Academy of Sciences of the United States of America, 105(9), 3374–3379.
10. Huang Q, Su H, Qi B, Wang Y, Yan K, Wang X, Li X, Zhao D. A SIRT1 Activator, Ginsenoside Rc, Promotes Energy Metabolism in Cardiomyocytes and Neurons. J Am Chem Soc. 2021 Jan 27;143(3):1416-1427.
11. Fang, Y., Wang, X., Yang, D., Lu, Y., Wei, G., Yu, W., Liu, X., Zheng, Q., Ying, J., & Hua, F. (2021). Relieving Cellular Energy Stress in Aging, Neurodegenerative, and Metabolic Diseases, SIRT1 as a Therapeutic and Promising Node. Frontiers in aging neuroscience, 13, 738686.
12. Hamaidi, I., Kim, S. Sirtuins are crucial regulators of T cell metabolism and functions. (2022) Exp Mol Med 54, 207–215.
13. Yamamoto M, Takahashi Y. (2018 Oct) The Essential Role of SIRT1 in Hypothalamic-Pituitary Axis. Front Endocrinol (Lausanne). 9:605.
Graphic: Modulating SIRT1 Signaling to Induce Optimal Aging
1. Hamaidi, I., Kim, S. Sirtuins are crucial regulators of T cell metabolism and functions. Exp Mol Med 54, 207–215 (2022).
2. Lee, I. H., Cao, L., Mostoslavsky, R., Lombard, D. B., Liu, J., Bruns, N. E., Tsokos, M., Alt, F. W., & Finkel, T. (2008). A role for the NAD-dependent deacetylase Sirt1 in the regulation of autophagy. Proceedings of the National Academy of Sciences of the United States of America, 105(9), 3374–3379.
3. Huang Q, Su H, Qi B, Wang Y, Yan K, Wang X, Li X, Zhao D. A SIRT1 Activator, Ginsenoside Rc, Promotes Energy Metabolism in Cardiomyocytes and Neurons. J Am Chem Soc. 2021 Jan 27;143(3):1416-1427.
4. Osum M, Serakinci N. Impact of circadian disruption on health; SIRT1 and Telomeres. DNA Repair (Amst). 2020 Dec;96:102993.
5. Yamamoto M, Takahashi Y. (2018 Oct) The Essential Role of SIRT1 in Hypothalamic-Pituitary Axis. Front Endocrinol (Lausanne). 9:605.
6. Zhou CH, Zhang MX, Zhou SS, Li H, Gao J, Du L, Yin XX. SIRT1 attenuates neuropathic pain by epigenetic regulation of mGluR1/5 expressions in type 2 diabetic rats. Pain. 2017 Jan;158(1):130-139.
7. Pandelides, Z., Thornton, C., Faruque, A. S., Whitehead, A. P., Willett, K. L., & Ashpole, N. M. (2020). Developmental exposure to cannabidiol (CBD) alters longevity and health span of zebrafish (Danio rerio). GeroScience, 42(2), 785–800.
Kang, S., Li, J., Yao, Z., & Liu, J. (2021). Cannabidiol Induces Autophagy to Protects Neural Cells from Mitochondrial Dysfunction by Upregulating SIRT1 to Inhibits NF-κB and NOTCH Pathways. Frontiers in cellular neuroscience, 15, 654340.
Wang, Z., Zheng, P., Chen, X. et al. Cannabidiol induces autophagy and improves neuronal health associated with SIRT1 mediated longevity. GeroScience (2022).
Bilkei-Gorzo, A., Albayram, O., Draffehn, A. et al. (2017) A chronic low dose of Δ9-tetrahydrocannabinol (THC) restores cognitive function in old mice. Nat Med 23, 782–787.
Pandelides, Z., Thornton, C., Lovitt, K. G., Faruque, A. S., Whitehead, A. P., Willett, K. L., & Ashpole, N. M. (2020). Developmental exposure to Δ9-tetrahydrocannabinol (THC) causes biphasic effects on longevity, inflammation, and reproduction in aged zebrafish (Danio rerio). GeroScience, 42(3), 923–936.
Liu, J., Godlewski, G., Jourdan, T., Liu, Z., Cinar, R., Xiong, K., & Kunos, G. (2019). Cannabinoid-1 Receptor Antagonism Improves Glycemic Control and Increases Energy Expenditure Through Sirtuin-1/Mechanistic Target of Rapamycin Complex 2 and 5’Adenosine Monophosphate-Activated Protein Kinase Signaling. Hepatology (Baltimore, Md.), 69(4), 1535–1548.
Zheng X, Sun T, Wang X. Activation of type 2 cannabinoid receptors (CB2R) promotes fatty acid oxidation through the SIRT1/PGC-1α pathway. Biochem Biophys Res Commun. 2013 Jul 5;436(3):377-81.
Hassanzadeh P, Hassanzadeh A (2012) The CB1 receptor-mediated endocannabinoid signaling and NGF: the novel targets of curcumin. Neurochemical Research 37: 1112–1120.
Zhang Z, Guo Y, Zhang S, et al. Curcumin modulates cannabinoid receptors in liver fibrosis in vivo and inhibits extracellular matrix expression in hepatic stellate cells by suppressing cannabinoid receptor type-1 in vitro. Eur J Pharmacol. 2013;721(1-3):133–140.
Endnotes: The Endocannabinoid System and SIRT1
1. Kang, S., Li, J., Yao, Z., & Liu, J. (2021). Cannabidiol Induces Autophagy to Protects Neural Cells from Mitochondrial Dysfunction by Upregulating SIRT1 to Inhibits NF-κB and NOTCH Pathways. Frontiers in cellular neuroscience, 15, 654340.
2. Wang, Z., Zheng, P., Chen, X. et al. Cannabidiol induces autophagy and improves neuronal health associated with SIRT1 mediated longevity. GeroScience (2022).
3. Liu, J., Godlewski, G., Jourdan, T., Liu, Z., Cinar, R., Xiong, K., & Kunos, G. (2019). Cannabinoid-1 Receptor Antagonism Improves Glycemic Control and Increases Energy Expenditure Through Sirtuin-1/Mechanistic Target of Rapamycin Complex 2 and 5’Adenosine Monophosphate-Activated Protein Kinase Signaling. Hepatology (Baltimore, Md.), 69(4), 1535–1548.
4. Zheng X, Sun T, Wang X. Activation of type 2 cannabinoid receptors (CB2R) promotes fatty acid oxidation through the SIRT1/PGC-1α pathway. Biochem Biophys Res Commun. 2013 Jul 5;436(3):377-81.
Endnotes: SIRT1 and the Endocannabinoidome
1. Zendedel E, Butler AE, Atkin SL, Sahebkar A. Impact of curcumin on sirtuins: A review. J Cell Biochem. 2018 Dec;119(12):10291-10300.
2. Hassanzadeh P, Hassanzadeh A (2012) The CB1 receptor-mediated endocannabinoid signaling and NGF: the novel targets of curcumin. Neurochemical Research 37: 1112–1120.
Zhang Z, Guo Y, Zhang S, et al. Curcumin modulates cannabinoid receptors in liver fibrosis in vivo and inhibits extracellular matrix expression in hepatic stellate cells by suppressing cannabinoid receptor type-1 in vitro. Eur J Pharmacol. 2013;721(1-3):133–140.
3. Yang Y, Duan W, Lin Y, Yi W, Liang Z, Yan J, Wang N, Deng C, Zhang S, Li Y, Chen W, Yu S, Yi D, Jin Z. SIRT1 activation by curcumin pretreatment attenuates mitochondrial oxidative damage induced by myocardial ischemia reperfusion injury. Free Radic Biol Med. 2013 Dec;65:667-679.
4. Sun Q, Jia N, Wang W, Jin H, Xu J, Hu H. (2014 May) Activation of SIRT1 by curcumin blocks the neurotoxicity of amyloid-β25-35 in rat cortical neurons. Biochem Biophys Res Commun. 448(1):89-94.
5. Sun Y, Hu X, Hu G, Xu C, Jiang H. Curcumin Attenuates Hydrogen Peroxide-Induced Premature Senescence via the Activation of SIRT1 in Human Umbilical Vein Endothelial Cells. Biol Pharm Bull. 2015;38(8):1134-41.
6. Freitas HR, Isaac AR, Malcher-Lopes R, Diaz BL, Trevenzoli IH, De Melo Reis RA. Polyunsaturated fatty acids and endocannabinoids in health and disease. Nutr Neurosci. 2018;21(10):695–714.
Calon F, Cole G. Neuroprotective action of omega-3 polyunsaturated fatty acids against neurodegenerative diseases: evidence from animal studies. Prostaglandins LeukotEssent Fatty Acids. 2007;77: 287–293.
Lafourcade M, Larrieu T, Mato S, Duffaud A, Sepers M, Matias I, et al. Nutritionalomega-3 deficiency abolishes endocannabinoid-mediated neuronal functions. NatNeurosci. 2011;14: 345–350.
Larrieu T, Madore C, Joffre C, Layé S. Nutritional n-3 polyunsaturated fatty acids deficiency alters cannabinoid receptor signaling pathway in the brain and associated anxiety-like behavior in mice. J Physiol Biochem. 2012;68: 671–681.
7. Hayakawa K, Mishima K, Nozako M, Hazekawa M, Aoyama Y, Ogata A, Harada K, Fujioka M, Abe K, Egashira N, Iwasaki K, Fujiwara M. (2007 Mar) High-cholesterol feeding aggravates cerebral infarction via decreasing the CB1 receptor. Neurosci Lett. 414(2):183-7.
8. Diaz-Ruiz, A., Di Francesco, A., Carboneau, B. A., Levan, S. R., Pearson, K. J., Price, N. L., Ward, T. M., Bernier, M., de Cabo, R., & Mercken, E. M. (2019). Benefits of Caloric Restriction in Longevity and Chemical-Induced Tumorigenesis Are Transmitted Independent of NQO1. The journals of gerontology. Series A, Biological sciences and medical sciences, 74(2), 155–162.
9. Yessenkyzy, A., Saliev, T., Zhanaliyeva, M., Masoud, A. R., Umbayev, B., Sergazy, S., Krivykh, E., Gulyayev, A., & Nurgozhin, T. (2020). Polyphenols as Caloric-Restriction Mimetics and Autophagy Inducers in Aging Research. Nutrients, 12(5), 1344.
10. Iside, C., Scafuro, M., Nebbioso, A., & Altucci, L. (2020). SIRT1 Activation by Natural Phytochemicals: An Overview. Frontiers in pharmacology, 11, 1225.
11. Lopez Trinidad, L. M., Martinez, R., Kapravelou, G., Galisteo, M., Aranda, P., Porres, J. M., & Lopez-Jurado, M. (2021). Caloric restriction, physical exercise, and CB1 receptor blockade as an efficient combined strategy for bodyweight control and cardiometabolic status improvement in male rats. Scientific reports, 11(1), 4286.
Endnotes: SIRT1 Cautions
1. Powell, M. J., Casimiro, M. C., Cordon-Cardo, C., He, X., Yeow, W. S., Wang, C., McCue, P. A., McBurney, M. W., & Pestell, R. G. (2011). Disruption of a Sirt1-dependent autophagy checkpoint in the prostate results in prostatic intraepithelial neoplasia lesion formation. Cancer research, 71(3), 964–975.
Ming, M., Shea, C. R., Guo, X., Li, X., Soltani, K., Han, W., & He, Y. Y. (2010). Regulation of global genome nucleotide excision repair by SIRT1 through xeroderma pigmentosum C. Proceedings of the National Academy of Sciences of the United States of America, 107(52), 22623–22628.
Kang YY, Sun FL, Zhang Y, Wang Z. SIRT1 acts as a potential tumor suppressor in oral squamous cell carcinoma. J Chin Med Assoc. 2018 May;81(5):416-422.
Leslie M. (2009). SIRT1 takes down tumors. The Journal of Cell Biology, 185(2), 178.
Yeung, F., Hoberg, J. E., Ramsey, C. S., Keller, M. D., Jones, D. R., Frye, R. A., & Mayo, M. W. (2004). Modulation of NF-kappaB-dependent transcription and cell survival by the SIRT1 deacetylase. The EMBO journal, 23(12), 2369–2380.
2. Niederer F, Ospelt C, Brentano F, Hottiger MO, Gay RE, Gay S, Detmar M, Kyburz D. SIRT1 overexpression in the rheumatoid arthritis synovium contributes to proinflammatory cytokine production and apoptosis resistance. Ann Rheum Dis. 2011 Oct;70(10):1866-73.
Lin Z, Yang H, Kong Q, Li J, Lee SM, Gao B, Dong H, Wei J, Song J, Zhang DD, Fang D. USP22 antagonizes p53 transcriptional activation by deubiquitinating Sirt1 to suppress cell apoptosis and is required for mouse embryonic development. Mol Cell. 2012 May 25;46(4):484-94.
Chen WY, Wang DH, Yen RC, Luo J, Gu W, Baylin SB. Tumor suppressor HIC1 directly regulates SIRT1 to modulate p53-dependent DNA-damage responses. Cell. 2005 Nov 4;123(3):437-48.
3. Lin, Z., & Fang, D. (2013). The Roles of SIRT1 in Cancer. Genes & cancer, 4(3-4), 97–104.
4. Niederer F, Ospelt C, Brentano F, Hottiger MO, Gay RE, Gay S, Detmar M, Kyburz D. SIRT1 overexpression in the rheumatoid arthritis synovium contributes to proinflammatory cytokine production and apoptosis resistance. Ann Rheum Dis. 2011 Oct;70(10):1866-73.
5. Lee, J., You, J. H., Kim, M. S., & Roh, J. L. (2020). Epigenetic reprogramming of epithelial-mesenchymal transition promotes ferroptosis of head and neck cancer. Redox biology, 37, 101697.
A £2.5 million study into the effects of cannabis on the brain has been launched by a London university.
The Cannabis & Me study will research environmental and biological factors behind the different effects people experience when using cannabis.
Dr Marta di Forti wants to investigate genetic interactions with the drug
King’s College London want 6,000 people to take part in the investigation, which would be the largest independent study of its kind.
Researchers said the funding from the Medical Research Council would help develop greater understanding of the drug, estimated to be used by 200 million people across the world.
More research is needed about how the drug interacts with the brain so doctors can be more confident when considering prescribing medical cannabis, said lead researcher, Dr Di Forti.
“Cannabis is consumed daily by many recreationally but also for medicinal reasons,” she said.
“But in the UK, the prescription of medicinal cannabis remains rare.
“Our study aims to provide data and tools that can make physicians in the UK and across the world more confident, where appropriate, in prescribing cannabis safely.”
The aim is to understand the link between a user’s biological makeup and the effect cannabis has on them.
Production of cannabis-infused medicine at the Government Pharmaceutical Organization in Thailand
Researchers will use a combination of virtual reality, psychological and cognitive analysis, and DNA testing.
They will also look at epigenetics in participants, which is how behaviour and environment can impact the way genes work.
Dr Di Forti said she was particularly interested in uncovering any markers connected to potential problems in users, for example mental health or social problems.
The team is now looking for participants between the ages of 18-45 living in the London area, who are either currently using cannabis or have used it less than three times or never before.
Experts agree that the use of marijuana is not causally linked to the use of other illicit substances
“This study is the first to use nationally representative data across all 50 states and the District of Columbia to comprehensively explore the broader impacts of RMLs [recreational marijuana laws], providing some of the first evidence on how marijuana legalization is affecting illicit drug use, heavy alcohol use, arrests for drug and non-drug offenses, and objectively-measured adverse drug-related events including drug-related overdose deaths and admissions into substance abuse treatment services. … [W]e find little compelling evidence to suggest that RMLs result in increases in illicit drug use, arrests for part I offenses, drug-involved overdoses, or drug-related treatment admissions for addiction.”Is recreational marijuana use a gateway to harder drug use and crime? National Bureau of Economic Research, 2021
“Marijuana use has been proposed to serve as a ‘gateway’ that increases the likelihood that users will engage in subsequent use of harder and more harmful substances, known as the marijuana gateway hypothesis (MGH). The current study refines and extends the literature on the MGH by testing the hypothesis using rigorous quasi-experimental, propensity score-matching methodology in a nationally representative sample. … Results from this study indicate that marijuana use is not a reliable gateway cause of illicit drug use. As such, prohibition policies are unlikely to reduce illicit drug use.”Is marijuana really a gateway drug? A nationally representative test of the marijuana gateway hypothesis using a propensity score matching design, Nature Communications, 2021
Sequentially, most consumers of illicit substances first experimented with either alcohol or tobacco
“Alcohol is the most commonly used substance, and the majority of polysubstance using respondents consumed alcohol prior to tobacco or marijuana initiation. Respondents initiating alcohol use in sixth grade reported significantly greater lifetime illicit substance use and more frequent illicit substance use than those initiating alcohol use in ninth grade or later. … Our results … assert that the earlier one initiates alcohol use, the more likely that they will engage in future illicit substance use.”Prioritizing alcohol prevention: Establishing alcohol as the gateway drug and linking age of first drink with illicit drug use, The Journal of School Health, 2016
Statistically, the overwhelming majority of people to try marijuana do not go on to use other illicit drugs, and most typically cease their use of marijuana by middle age
In jurisdictions where marijuana is legally accessible, adults typically report decreasing their use of other controlled substances. In this sense, marijuana appears to act more as a potential ‘exit drug’ rather than as an alleged ‘gateway’
“This study assessed (1) trends in alcohol, nicotine, and nonprescribed pain reliever use and (2) changes in associations of cannabis use with these other substances among young adults in Washington State after nonmedical cannabis legalization. …Contrary to concerns about spillover effects, implementation of legalized nonmedical cannabis coincided with decreases in alcohol and cigarette use and pain reliever misuse. The weakening association of cannabis use with the use of other substances among individuals ages 21-25 requires further research but may suggest increased importance of cannabis-specific prevention and treatment efforts.”Trends in alcohol, cigarette, e-cigarette, and nonprescribed pain reliever use among young adults in Washington state after legalization of nonmedical cannabis, Journal of Adolescent Health, 2022
“[F]indings on cannabis substitution effect and the biological mechanisms behind it strongly suggest that cannabis could play a role in reducing the public health impacts of prescription and non-prescription opioids. … The growing body of research supporting the medical use of cannabis as an adjunct or substitute for opioids creates an evidence-based rationale for governments, health care providers, and academic researchers to consider the implementation and assessment of cannabis-based interventions in the opioid crisis.”Rationale for cannabis-based interventions in the opioid overdose crisis, Harm Reduction Journal, 2017
“Among respondents that regularly used opioids, over three-quarters (76.7%) indicated that they reduced their use since they started medical cannabis. This was significantly ( p < 0.0001) greater than the patients that reduced their use of antidepressants (37.6%) or alcohol (42.0%). Approximately two-thirds of patients decreased their use of anti-anxiety (71.8%), migraine (66.7%), and sleep (65.2%) medications following medical cannabis.”Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep, Journal of Psychopharmacology, 2017
In clinical settings, marijuana use is associated with reduced cravings for cocaine and opiates
“In this longitudinal study, we observed that a period of self-reported intentional use of cannabis … was associated with subsequent periods of reduced use of crack [cocaine]. … Given the substantial global burden of morbidity and mortality attributable to crack cocaine use disorders alongside a lack of effective pharmacotherapies, we echo calls for rigorous experimental research on cannabinoids as a potential treatment for crack cocaine use disorders.”Intentional cannabis use to reduce crack cocaine in a Canadian setting: A longitudinal analysis, Addictive Behaviors, 2017
We wanted to take a closer look at the science behind using CBD for bipolar affective disorder.
The National Mental Health Institute estimates 4.4 percent of adults in the United States will be given a diagnosis of bipolar affective disorder (BPAD) in their lifetime. Adults with BPAD experience the highest rate of impairment among psychiatric patients; an estimated 82.9 percent suffer from severe disablement.
Bipolar affective disorder and its variants can be treatment resistant, which may explain the high rate of disability. Anecdotal evidence, supported by preliminary studies, suggest that cannabinoids have the potential to improve the symptoms of BPAD in some individuals by regulating the endocannabinoid system.
WHAT IS BIPOLAR AFFECTIVE DISORDER?
Bipolar affective disorder is a mental illness that causes significant changes in mood, motivation and energy. A process known as cycling, which involves periods of euphoria (manic episodes) followed by hopelessness (depressive episodes), is a hallmark of the illness.
There are four variants of bipolar affective disorder: bipolar I, bipolar II, cyclothymic disorder and bipolar spectrum disorders. The severity and frequency of symptoms are used to determine which variant is diagnosed. Bipolar I is the most severe form of the disease.
SYMPTOMS OF MANIC EPISODES
Manic episodes, sometimes referred to as mania, are characterized by exaggerated self-esteem, insomnia, racing thoughts and abnormal speech, inability to focus, and impulsive behaviours. True manic episodes only affect those diagnosed with bipolar I disorder. However, patients with other variants of BPAD experience hypomania, a less severe form of mania.
Although mania is considered to be the “high” stage of BPAD, it can have disastrous consequences. Many manic episodes result in hospitalization, psychotic symptoms or grave impairment (e.g., risky behaviour leading to legal trouble). Untreated manic episodes can develop into psychosis.
SYMPTOMS OF DEPRESSIVE EPISODES
Depressive episodes mimic a severe form of depression known as major depressive disorder. Symptoms can include feelings of sadness, emptiness, hopelessness, and loss of interest in activities. Additional traits of depressive episodes are changes in sleep patterns and appetite, trouble concentrating, feelings of worthlessness or guilt, and suicidal thoughts or attempts.
This cycle of bipolar disorder is the “low” point of the disease. Like mania, depressive episodes vary in severity depending on which variant of bipolar disorder is present. Patients with Bipolar I disorder may have what are known as mixed episodes, during which they show signs of both mania and depression.
CONVENTIONAL TREATMENTS OF BIPOLAR DISORDER
Prescription drugs used in conjunction with psychotherapy can help alleviate symptoms of BPAD in most patients. However, bipolar affective disorder can be treatment-resistant, making it difficult to manage in some people. Treatment-resistant BPAD is cause for concern, as up to 50 percent of individuals diagnosed will attempt suicide at least once in their lives.
Medications prescribed for BPAD include anticonvulsants, antimanic drugs and antidepressants. Use of antidepressants alone can lead to the onset of mania or rapid cycling. Mood stabilizers or anticonvulsants are often taken to negate these possible side effects.
The only pharmaceutical shown to have a consistent, positive effect on suicide rates in bipolar patients is lithium. However, newer research has shown there may be a possibility to control BPAD through manipulating the endocannabinoid (EC) system. These are the neurotransmitters responsible for binding cannabinoid proteins to receptors.
ENDOCANNABINOID SYSTEM DYSFUNCTION AND BPAD
The endocannabinoid system, discovered in the mid-1990s, is comprised of two receptors, CB1 and CB2. Cannabinoids, a type of compound found in both the human body and cannabis plants, bind to these receptors to alter brain function. Endocannabinoids are neurotransmitters produced naturally in the body, while phytocannabinoids are found in cannabis plants.
Postmortem studies have found that brains of patients diagnosed with mental illness, including BPAD variants, show abnormalities in the endocannabinoid system. A similar study, conducted using brain slices from mice, showed dysfunctional CB2 receptors inhibited the release of serotonin, suggesting a healthy EC system helps to regulate mood.
An investigation of endocannabinoid gene variants in 83 patients with major depressive disorder (MDD), 134 with BPAD, and 117 healthy control participants found two marked differences in the patients afflicted with MDD and BPAD. Specifically, the CB1 receptor (CNR1) and fatty acid amide hydrolase (FAAH) genes of the ill participants were found to be abnormal when compared to the control group.
REGULATING THE EC SYSTEM WITH PHYTOCANNABINOIDS
Because of the distribution of endocannabinoid receptors throughout the brain, many of the areas they affect overlap with regions thought to be responsible for BPAD, along with other mental illnesses. Studies have shown patients with specific abnormalities in the CNR1 gene are at a higher risk of being resistant to pharmacological treatment, leaving them more vulnerable to the effects of bipolar affective disorder.
For these patients, phytocannabinoids could provide a way to manipulate the EC system and regulate the level of chemicals traditionally targeted by pharmacological medications. As always with hemp and cannabis research, these studies are still preliminary. More research will be needed to prove whether CBD and other cannabinoids can help treat bipolar affective disorder.
ANANDAMIDE AND THC
Anandamide, called the bliss molecule, is naturally produced in the body and is similar in molecular structure to THC. Both anandamide and THC bind to CB1 receptors, altering areas of the brain responsible for memory, concentration, movement, perception, and pleasure.
FAAH genes are responsible for activating anandamide; indicating people with FAAH gene mutations may not have the appropriate levels of anandamide in the brain. Supplementing brains deficient in anandamide with THC may help restore chemical balances. Theoretically, this could alleviate cycling between manic and depressive phases.
CANNABIDIOL (CBD)
Cannabidiol has been shown to inhibit serotonin reuptake in rats, suggesting it repairs abnormalities in CB1 receptors found to inhibit release in mice. If CBD functions the same in human brains, it could provide an alternative to conventional antidepressants, especially for individuals with treatment-resistant BPAD.
A randomized clinical trial found CBD reduces abnormal brain function in regions associated with psychosis, implying it may have therapeutic effects on symptoms associated with the manic phase of BPAD. If CBD regulates both depressive and manic symptoms, it could help treat individuals who do not react well to lithium.
OTHER CANNABINOIDS
Cannabis is a complex compound, made up of over 500 chemicals. Over 100 of these compounds are suspected to be cannabinoids. There is little information on the effects of these chemicals, apart from CBD and THC, because few studies have focused on determining what reactions they produce in the EC system.
Among cannabinoids that have already been isolated, CBG and CBCV seem to show a potential for treating mood disorders, such as depression. Further study may help isolate more of these chemicals and determine what effect they have on the EC system.
USING CBDS & OTHER CANNABINOIDS FOR BIPOLAR AFFECTIVE DISORDER
CBD rarely causes adverse reactions. Still, there are risks associated with both conventional methods of treatment and using cannabis derivatives as treatment. The most dangerous side effect of any treatment for BPAD is the potential worsening of symptoms.
Individuals experiencing symptoms of bipolar affective disorder, or previously diagnosed with any of the variants, should consult with a medical professional before starting or changing treatment. Even those who present with treatment-resistant variations of the disease can benefit from traditional methods (such as psychotherapy).
Regulating the EC system through phytocannabinoids may provide a way to alleviate symptoms in those with treatment-resistant BPAD. Further clinical trials in humans are needed to validate preliminary data, but the future of cannabinoids as a BPAD treatment looks promising.
Source: HempToday.net | Author: Hemp Today | June 22, 2022
EIHA projects GmbH, a consortium of the European Industrial Hemp Association (EIHA), said research it is currently conducting on the safety of CBD will meet the expectations of the European Food Safety Authority (EFSA).
Concern about safety on the part of EFSA “is definitely not a surprise and 100% in line with our approach,” EIHA said in a statement.
EFSA earlier this month said it had identified gaps in research regarding the effects of CBD on humans, declaring “the safety of CBD as a novel (new) food cannot currently be established.”
The EIHA consortium is spending €2.5 to €3 million on extensive toxicology and clinical research regarding CBD and THC which will be the basis for its novel food applications, which cover isolates and full-spectrum formulations.
Pooling resources
“We decided in 2021 to pool the resources of more than 100 companies and work . . . on a serious and solid submission, anticipating the scientific gaps indicated by EFSA,” EIHA said.
While EFSA has not concluded that CBD consumption is dangerous, the agency said in a statement issued earlier this month that research currently available on the compound’s effects on the liver, gastrointestinal tract, endocrine system, nervous system, and on psychological well-being is insufficient.
The EFSA statement was a response to the European Commission, which sought input from the agency’s experts regarding the safety of CBD. The Commission has said CBD can be classified as a new or “novel” food if it meets relevant provisions in EU food legislation.
Cutting costs
EIHA formed the consortium as a way to reduce the cost of the EU’s novel food approval procedure to its members. The Association estimates the cost of getting a single product approved under novel food rules as ranging from €350,000 to €500,000 per product.
Participation in the EIHA consortium, structured in two categories, significantly reduces those costs. In the first category, producers of hemp biomass and raw materials, makers of processed extracts, premixes, oils, and isolates as well as service providers pay fees according to an eight-tier payment structure which ranges from €20,000 for those with CBD-related income of €1 million or less, up to €330,000 for those with income of €50 million or more. Consortium participants are also required to join the EIHA on a parallel rate scale that ranges from €2,500 to €25,000.
Under a companion 12-tier sublicensing program for white-label operators, fees range from €1,800 for companies with income of €10,000 or less up to €405,000 for those with income of €50 million or more.
Novel food in the EU
Europe’s novel food rules were created to control new, genetically or synthetically produced food products before market entry. Under the guidelines, novel foods are defined as those that were not consumed to a significant degree in the EU before May 15, 1997. If a food is considered novel it must undergo a pre-market safety assessment under EFSA before it can be legally marketed in the EU.
ChemSafe, an Italian consultancy that has experience in the chemical, pharmaceutical, biocides, agrochemical, cosmetics, medical devices and food sectors, is heading the science-based analysis of CBD and THC on behalf of EIHA.
EFSA has scheduled an information session June 28, during which agency representatives will answer questions and provide guidance to current novel food applicants regarding the research gaps identified. A total of 19 CBD applications are now before the agency.
A new study performed by Cannabotech has demonstrated that the company’s range of Integrative-Colon products may be an effective colon cancer treatment, killing 90% of colon cancer cells in a cell model study.
Cannabotech is a biotechnology company pioneering oncological products comprised of cannabis and mushroom extracts. In a recent cell model study, the company has demonstrated that its Integrative-Colon products, which are based on an array of cannabinoids from the cannabis plant and various mushroom extracts, eliminated over 90% of colon cancer cells. The findings offer an exciting prospect for the future of colon cancer treatment.
How did the Integrative Colon products perform?
For their study, the researchers analysed the effectiveness of the Integrative Colon products on a range of colon cancer subtypes, representing different molecular changes that a prevalent in these cancer subtypes. The team compared the composition of the products with the activity of each cannabinoid individually.
The results suggested that the composition of the Integrative Colon products was more effective than each cannabinoid individually, highlighting a strong synergy between the active ingredients. These findings back up claims from Cannabotech that to achieve an effective cannabis colon cancer treatment, it is essential to amalgamate a defined, accurate, and science-based formula that cannot be achieved in any cannabis strain that exists in nature.
Additionally, the study showed the different effects of each cannabinoid on distinct colon cancer subtypes. This echoes the essential need for a individualised approach for patients’ health needs, such as the personalised technology already developed by Cannabotech that will soon hit the market in the UK, US, and Israel at the end of 2022.
The mushroom extracts in the products contain an enriched and high concentration of an active substance called PSK that is extracted from the Trametes mushroom. PSK is known for its anti-cancer properties and has been approved as an oncology treatment in Taiwan, Japan, and South Korea.
Future steps
The researchers are now looking to assess the effectiveness of the formula in combination with standard chemotherapies. In addition, the team plan to combine the cannabinoid formula with the mushroom Cyathus Striatus as part of the botanical drug development project.
Elhanan Shaked, the CEO of Cannabotech, commented: “This is a significant milestone in Cannabotech’s growth to becoming a leader in integrative oncology medicine. The integrative products developed by Cannabotech are intended for use in combination with chemotherapy treatment to reduce its side effects. Cannabotech’s solutions will be launched in Israel and the US towards the second half of 2022, while the company’s goal is to define a new standard for the medical cannabis industry.”
Professor Tami Peretz, Senior Oncologist, said: “Colon cancer is one of the most common tumours today, with a significant proportion of patients currently treated with integrative therapies, in combination with traditional methods, including the administration of medical cannabis. Cannabotech’s Integrative products are unique in that they are designed to standards similar to those of the pharmaceutical industry and incorporate many active ingredients. The company’s products have demonstrated impressive and very promising efficacy in colon culture cells tested in the laboratory. Based on these experiments, there is room to perform animal studies and, in the future, to examine the possibility of incorporating these products in colorectal cancer patients.”
Isaac Angel, Cannabotech’s pharmacological consultant, said: “The significant synergistic effect demonstrated by the combination of active ingredients eliminated over 90% of all types of cancer cells used in the study. Furthermore, this was achieved without the presence of THC, which is the cannabinoid substance producing the “high” effect, whereas each of the other cannabinoids tested individually demonstrated different effects on the various cell types. We are encouraged by these results, which constitute another important milestone in proving the scientific feasibility of the products and highlight the need for medical care customisation. We shall continue to work to provide a cure for patients.”